Lumbar Lordosis: What the Lower-Back Curve Looks Like
Lumbar lordosis is the natural inward curve of the lower spine — the gentle hollow you can see above the buttocks in a side-view photo. Everyone has some; it is a normal feature of the human spine, not a problem in itself. What varies from person to person is the depth of that curve: a typical curve, an exaggerated one (hyperlordosis), or a flattened one (hypolordosis). The depth of the lumbar curve is a postural description, not a diagnosis, and it should be interpreted together with the full clinical picture. This guide explains what lumbar lordosis looks like in 2D photos, how the curve connects to pelvic tilt, how to take a usable side view, and when the photo signs are worth discussing with a clinician.
- Lumbar lordosis = the normal inward curve of the lower back. Everyone has one; only the depth varies.
- A deep curve is hyperlordosis (“swayback” look); a flat curve is hypolordosis (“flat back” look). Both are descriptions, not diagnoses.
- The lumbar curve tracks with pelvic position: anterior pelvic tilt deepens it, posterior pelvic tilt flattens it.
- Most visible from the side view of a clean full-body photo, with the camera at hip height and 2–3 meters away.
- A strongly flattened or exaggerated curve combined with persistent pain, stiffness, or a recent change in a child or teen is worth discussing with a licensed clinician.
What lumbar lordosis is
Lumbar lordosis is the inward curve of the lower section of the spine — the five lumbar vertebrae that sit between the ribcage and the pelvis. Viewed from the side, a healthy lumbar spine curves gently toward the front of the body, creating the small hollow most people can feel in their lower back. This curve is normal and necessary: it helps the spine absorb load, balance the weight of the upper body over the pelvis, and keep the head positioned over the hips.
Because the curve is normal, the word lordosis by itself does not describe a problem. Everyone has lumbar lordosis. The clinically meaningful question is about degree. A curve that sits within the typical range is simply normal lordosis. A curve that is much deeper than typical is called hyperlordosis, sometimes described colloquially as “swayback”. A curve that is much shallower than typical — a lower back that looks unusually straight — is called hypolordosis or, informally, “flat back.”
Some readers will encounter the same anatomy under related terms. Lumbosacral lordosis refers to the same lower-spine curve, emphasizing the junction where the lumbar spine meets the sacrum. Loss of lumbar lordosis is the radiology phrasing for a flattened curve. These all describe the same structure seen from different angles.
It helps to place lordosis next to its opposite, kyphosis. Lordosis is an inward curve; kyphosis is an outward one. The lower back and the neck curve inward (lordosis); the upper back curves outward (thoracic kyphosis). A healthy spine alternates between these curves, and all of them are normal in moderation. The companion guide on the 17 posture metrics covers how each spinal curve is described in a report.
A few framing notes matter here, and they echo every article in this series. The depth of the lumbar curve is a postural description, not a diagnosis. The Cleveland Clinic notes that most lordosis is not severe enough to cause symptoms or require treatment. Throughout this article, the focus stays on what the curve looks like in a 2D side photo and how to interpret what you see.
How much lumbar curve is normal
There is no single “correct” lumbar curve. Healthy adults show a wide range, and the typical range is broad enough that two people with visibly different lower backs can both be entirely normal. Radiographic studies that measure the lumbar curve as a Cobb angle report typical values spanning roughly 20 to 60 degrees across healthy adults, with meaningful variation by age, sex, and population. That width is the point: a curve that looks a little deep or a little flat in a photo is usually still within the normal envelope.
That observation matters for how to read a photograph. Seeing a moderately deep or moderately shallow lumbar curve in a side photo does not, on its own, mean anything is wrong. This is a relatively common finding and is often asymptomatic, but it should be interpreted together with the full clinical picture. A person with a slightly exaggerated curve and no pain, no movement limitations, and no functional concerns is statistically closer to the norm than to an outlier.
Where the curve becomes more meaningful is when it is strongly outside the typical range — a clearly deep arch or a clearly flattened lower back — AND it co-occurs with persistent low-back pain, stiffness, or movement restrictions. A specific situation warrants earlier attention: a curve that changes noticeably in a child or teenager during growth, which is worth a clinical look regardless of pain. In all of these situations the photo serves as one data point in a broader conversation — never the diagnosis itself.
Several factors are commonly associated with a deeper or shallower lumbar curve in observational studies: habitual sitting posture, pelvic position, and patterns of muscle length around the hips and trunk. Whether any of these cause a particular curve in any given person is a research question that goes beyond a postural photograph. For most practical purposes, the right mindset is: normal curve with wide variation, sometimes worth a closer clinical look, often worth nothing more than noticing.
What lumbar lordosis looks like in 2D photos
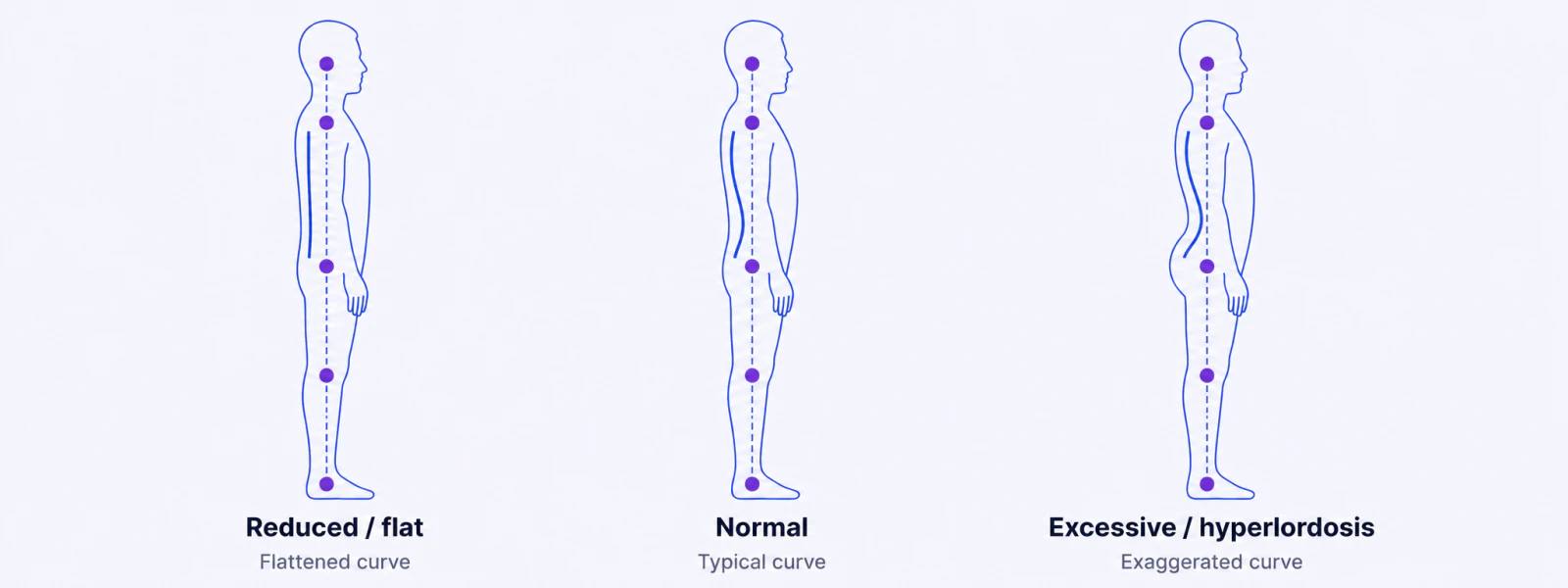
The most reliable place to read the lumbar curve is a side-view photograph taken at roughly hip height, with the whole body in frame and a clean background behind the subject. From that angle, the curve appears as the contour of the lower back between the ribcage and the top of the buttocks. Three patterns are worth recognizing.
A normal lumbar curve shows a gentle, smooth inward sweep. The lower back moves inward from the bottom of the ribcage, reaches its deepest point in the mid-lumbar region, and returns outward toward the buttocks. The hollow is present but not dramatic, and the overall line from shoulders to hips looks balanced.
Hyperlordosis — an exaggerated curve — shows a deeper, more pronounced hollow. The arch above the buttocks looks accentuated, the buttocks tend to project backward, and the abdomen may appear to tilt forward. This is the look people describe as “swayback.” On a side photo, the inward curve is visibly sharper than a gentle sweep.
Hypolordosis — a reduced curve — shows a flattened lower back. The usual hollow is shallow or nearly absent, and the lower spine looks unusually straight from the side. The buttocks tend to tuck under rather than project. This is the look people describe as “flat back.”
Several common photo conditions distort or hide the curve. A camera held above hip height can make the lower back look flatter than it is; a camera below hip height can exaggerate the arch. Loose drape-style clothing hides the contour entirely. Photos taken from a slight three-quarter angle rather than a true side view make the curve unreliable to judge. The next section on capture protocol covers how to avoid these errors.
It is worth emphasizing what the visible curve is not. It is not a measurement of the underlying spinal angle the way a radiograph (a Cobb-angle measurement) would measure it. It is a surface-contour pattern that suggests the underlying curve. Clothing, body composition, breathing phase, and the moment when the photo is captured all influence what shows up. The visual signal is genuinely useful, especially for trending over time in the same person under the same conditions — but it is a screening signal, not a diagnostic measurement.
Lordosis and pelvic tilt — the connection
The lumbar curve does not move on its own. It is mechanically linked to the position of the pelvis sitting directly beneath it. When the pelvis rotates, the lower-back curve follows. This is why the lumbar curve and pelvic tilt are best read together in a side photo — they are two views of the same underlying posture.
When the pelvis tips forward — anterior pelvic tilt — the top of the sacrum rotates downward at the front, and the lumbar spine deepens its curve to compensate. The result trends toward hyperlordosis: a deep arch and projecting buttocks. When the pelvis tips backward — posterior pelvic tilt — the sacrum rotates upward at the front, and the lumbar curve flattens. The result trends toward hypolordosis: a flat lower back and tucked buttocks.
| Reduced lordosis Flat back | Normal lordosis Typical curve | Excessive lordosis Hyperlordosis | |
|---|---|---|---|
| Lower-back curve depth | Shallow / flat | Gentle inward curve | Deep / pronounced |
| Associated pelvic tilt | Posterior tilt | Neutral | Anterior tilt |
| Buttocks appearance | Tucked under | Normal | Projects backward |
| Everyday label | "Flat back" | "Neutral" | "Swayback" |
This connection is practically useful. If a side photo shows a deep lumbar arch, looking at the pelvis usually reveals an anterior tilt, and vice versa. Reading them together gives a more complete picture than either one alone — and it explains why the pelvic-tilt guides and this lumbar-curve guide describe the same photographs from two directions.
The takeaway: knowing where someone’s curve sits on this spectrum, and how it relates to their pelvis, is more useful than placing them in a single category. A person whose photo signals “slightly deep curve” is not in the same situation as someone whose photo signals “strongly exaggerated curve with pain and stiffness.”
How to take a side photo to see your own lumbar curve
A photograph that reliably reveals the lumbar curve follows a short capture protocol. Most distortion comes from the camera, not from the body — small changes in camera height, angle, or distance can make the same person’s curve look deeper or flatter than it actually is.
The protocol is straightforward:
- Background. Stand against a plain wall or a flat surface free of clutter. Avoid backgrounds with horizontal lines that compete visually with the back contour.
- Body position. Stand sideways to the camera, weight evenly distributed on both feet, arms relaxed at the sides. Avoid pressing the arms against the hips or putting hands in pockets. Look straight ahead, not down or up.
- Camera position. The camera should sit at approximately hip height, not above or below. A tripod or a stack of books works. A phone propped against something stable is fine.
- Camera distance. Two to three meters away. Closer than that introduces lens distortion that exaggerates whichever body part is closest to the camera.
- Framing. The whole body should be in the frame, with the hip approximately in the vertical center of the photo. Heads cut off, feet cut off, or hips off-center will make later comparisons unreliable.
- Camera level. Use a phone’s built-in level indicator or a level app. A tilted camera makes every angle in the photo unreliable.
- Clothing. Close-fitting, athletic, or undergarments work best. Loose drape clothing hides the lower-back contour completely. The goal is to see body contours, not fabric drape.
- Pose. Stand naturally. “Performing good posture” defeats the point of the photograph. Stand the way you stand when you are not thinking about it.
For self-screening, taking the same photo every few weeks under the same conditions is more informative than a single grade. The PosturaScreen sample report shows what a clinical report based on this kind of capture looks like, and the methodology page documents how each metric is computed from the keypoints in the photo.
Three common mistakes account for most “my photo looks weird” results: (1) the camera was held by another person at chest height instead of being mounted at hip height; (2) the subject was wearing baggy or wrinkled clothing; (3) the subject “fixed” their posture before the photo was taken. Re-shooting under controlled conditions usually resolves these.
How PosturaScreen estimates lumbar lordosis from photos
PosturaScreen, the product behind this article, reports lumbar lordosis as one of its 17 posture metrics. The calculation is a surface-curvature estimate derived from the angle between the mid-back and hip keypoints relative to the trunk line — in other words, it reads the contour of the lower back from the visible landmarks in a side photo. The system does not measure the true spinal Cobb angle; it estimates a 2D surface signal from visible surface landmarks.
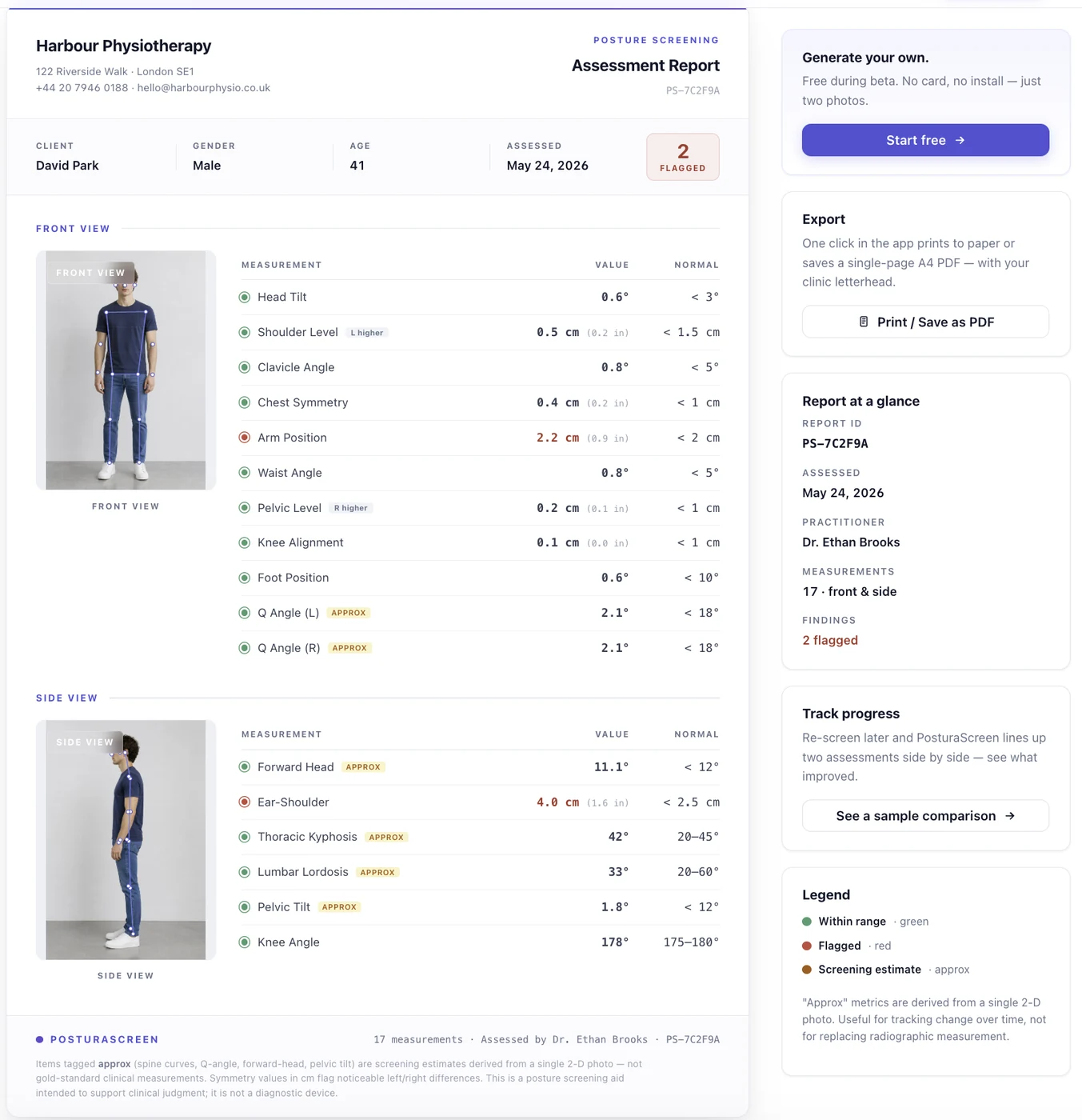
approx because a 2D surface estimate differs from a radiographic Cobb angle.In every report, this metric carries an approx tag — it is one of five metrics (forward head, thoracic kyphosis, lumbar lordosis, pelvic tilt, and Q-angle) that estimate a 3D angle or a spinal curve from a flat 2D photo. The tag is honest about what the number represents. The geometric calculation reliably captures the surface relationship of the lower back in the photo. It does not capture the underlying spinal curve the way a radiograph would, because surface contour is influenced by clothing, body composition, and breathing phase — none of which appear on an X-ray, the gold standard for spinal-curve measurement.
The supporting research is consistent on this point. Photographic postural angles are highly repeatable across raters and across repeated sessions (Hazar et al., 2015; Mylonas et al., 2025), and AI-based 2D posture estimates correlate strongly with radiographic measures without replacing them (Park et al., 2025). That is the exact basis for reporting a useful screening number while tagging it approx.
The practical value of this number is not absolute clinical grading. The practical value is trending in the same person under consistent capture conditions. A lumbar curve reading today is not directly comparable to someone else’s reading taken under different conditions, but it is comparable to that same person’s reading six weeks later, if both photos were taken with the same setup. The full mathematical definition of every metric lives on the PosturaScreen methodology page.
When to talk to a clinician about lumbar lordosis
A side photo showing a deeper or flatter lumbar curve does not require a clinical visit on its own. As noted earlier, the normal range is wide, and the curve depth alone does not prove anything is harmful or clinically significant.
The signal becomes worth a clinician’s attention when it co-occurs with one or more of the following:
- Persistent low-back, hip, or leg pain that does not resolve with simple rest or that recurs with activity.
- Movement limitations — difficulty standing, walking, or bending comfortably, or stiffness that interferes with normal activity.
- A noticeable change during growth — a curve in a child or teenager that becomes visibly deeper or flatter over months, which is worth a clinical look regardless of pain.
- Postural concerns paired with neurological symptoms — any numbness, weakness, or radiating pain into the legs. These warrant clinical evaluation independent of the curve.
Several professional groups are positioned to integrate a photo signal with the rest of someone’s clinical picture: licensed physiotherapists, chiropractors, sports-medicine physicians, and orthopedic specialists. They can perform a physical examination, take a history, and — when warranted — order imaging that measures the spinal curve directly. OrthoInfo from the American Academy of Orthopaedic Surgeons is a reasonable starting point for understanding when persistent musculoskeletal concerns warrant clinical evaluation.
What a photograph cannot do is replace any of that. A photograph is a snapshot of surface contour at a moment in time. It does not measure the spinal curve, pain, strength, or tissue health, and it does not capture the dozens of other things a clinician integrates into an assessment.
PosturaScreen is built as a screening and tracking tool. It is not a diagnostic device, and it does not provide medical advice. The information in this article is educational. For specific concerns about posture or musculoskeletal health, the right next step is a conversation with a qualified healthcare professional.
Frequently asked questions
What does lumbar lordosis look like?
Lumbar lordosis is the natural inward curve of the lower spine, visible from the side as a gentle hollow above the buttocks. A normal lordosis is a moderate curve. An excessive curve (hyperlordosis) looks like a deep, pronounced arch with the buttocks projecting backward; a reduced curve (hypolordosis or “flat back”) looks flattened, with the lower back appearing straight. The curve depth is what changes.
Is lumbar lordosis normal?
Yes. Lumbar lordosis is a normal, healthy feature of the human spine — everyone has some. The lower spine is supposed to curve gently inward. The question is never whether you have lumbar lordosis, but whether the curve is within the typical range, exaggerated (hyperlordosis), or reduced (flattened). All three are postural descriptions, not diagnoses on their own.
What is the difference between lordosis and kyphosis?
Lordosis is an inward curve of the spine; kyphosis is an outward curve. The lower back (lumbar) and the neck (cervical) curve inward — lordosis. The upper back (thoracic) curves outward — kyphosis. Both are normal in moderation. The terms only describe a concern when the curve is much larger or smaller than typical, which is when a clinician interprets it alongside symptoms.
What’s the connection between lumbar lordosis and pelvic tilt?
The pelvis and the lower-back curve move together. Anterior pelvic tilt (pelvis tipped forward) deepens the lumbar curve toward hyperlordosis. Posterior pelvic tilt (pelvis tipped backward) flattens the lumbar curve toward hypolordosis. In a side photo, the depth of the lower-back curve and the angle of the pelvis are two views of the same underlying posture.
Can a 2D photo measure lumbar lordosis?
A 2D side photo reliably shows the appearance of the lower-back curve and is useful for tracking change in the same person over time. It does not measure the underlying spinal curve the way a radiograph (Cobb angle) does, because surface contour is influenced by clothing, body composition, and breathing phase. That is why PosturaScreen tags lumbar lordosis approx in every report.
When should someone see a clinician about lumbar lordosis?
When a visibly flattened or exaggerated lower-back curve in side photos occurs alongside persistent pain, stiffness, or movement limitations — or when the curve changes noticeably in a child or teenager — it is worth consulting a licensed physiotherapist, physician, or chiropractor. They can integrate the photo signal with an examination and history. PosturaScreen is a screening and tracking tool, not a diagnostic device.
This article was prepared by the PosturaScreen editorial team for posture education. It is not medical advice and is not a substitute for a clinical evaluation. PosturaScreen is a screening and tracking tool, not a diagnostic device. If you have concerns about your posture or musculoskeletal health, consult a licensed healthcare professional. See our editorial standards for how this article was written and reviewed.