Posterior Pelvic Tilt: What It Looks Like in 2D Photos
Posterior pelvic tilt (PPT) is a postural pattern where the back of the pelvis drops and the front rises, flattening the natural curve of the lower back and tucking the hips under the body. From the side, it shows up as a flattened lower-back contour, a waistline that tilts upward at the front, and buttocks that appear tucked in rather than projecting. This is a relatively common finding and is often asymptomatic, but it should be interpreted together with the full clinical picture. This guide explains what PPT looks like in 2D photos, how to take a usable side view, the difference between PPT and anterior pelvic tilt, and when the photo signs are worth discussing with a clinician.
- PPT = back of the pelvis drops, front rises → flattened lower-back curve and an upward-tilted waistline.
- Most visible from the side view of a clean full-body photo, with the camera at hip height and 2–3 meters away.
- PPT is a postural pattern, not a diagnosis. It is relatively common and often asymptomatic, but it should be interpreted together with the full clinical picture.
- A 2D photo lets a person track changes in pelvic position over weeks or months — that is the strongest use case, not a one-time grade.
- A strong PPT signal combined with persistent pain, stiffness, or movement limitations is worth discussing with a licensed physiotherapist, physician, or chiropractor.
What posterior pelvic tilt is
Posterior pelvic tilt (PPT) describes a postural pattern where the back of the pelvis drops and the front of the pelvis rises. Viewed from the side, the pelvis rotates as a unit so the top of the iliac crests tilts backward and downward, while the front tilts upward. This rotation flattens the natural curve of the lower back — reducing what clinicians call lumbar lordosis — and tucks the hips under so they sit beneath or slightly behind the line of the shoulders.
Some readers will encounter the same pattern under different names. A tucked pelvis, a posterior pelvic rotation, and a generic flat-back appearance in the lumbar region all refer to the same underlying rotation. The term flat back is sometimes used more broadly to describe a whole-spine posture, but the lumbar flattening that defines PPT is its most consistent visible feature.
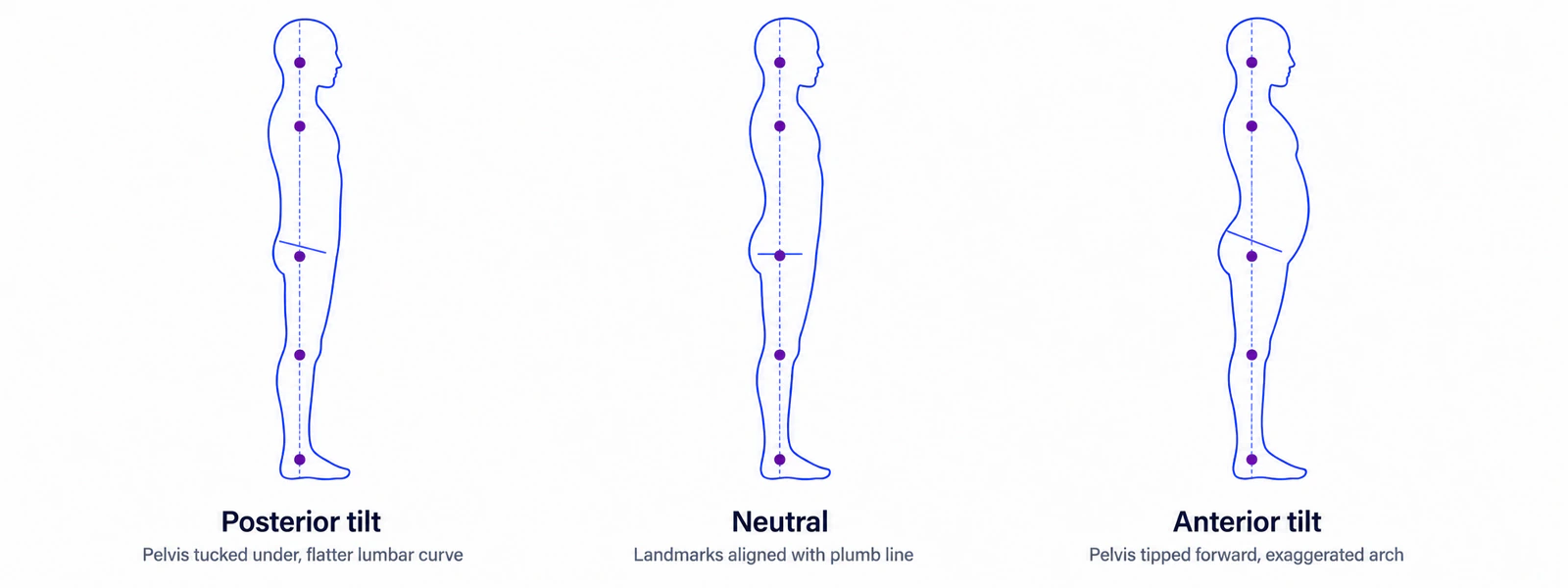
The opposite pattern, anterior pelvic tilt (APT), happens when the top of the pelvis rotates forward. The lower-back curve becomes pronounced, the hips appear ahead of the shoulders, and the buttocks stick out. A neutral pelvic position sits between the two extremes, with the lower back showing a normal lordotic curve but without the exaggerated arch of APT or the flatness of PPT.
A few framing notes matter here. PPT is a postural pattern, not a diagnosis. The phrase appears in physiotherapy literature, athletic-training material, and consumer health content because the visible signs are easy to identify — not because every visible PPT is medically significant. The Cleveland Clinic, for example, describes pelvic tilt as a description of pelvic position relative to neutral, separate from any judgment about whether it requires intervention.
Throughout this article, the focus stays on what PPT looks like in a 2D side photo and how to interpret what you see. PosturaScreen, the product behind this blog, estimates a pelvic tilt angle from photo landmarks and tags it approx because surface-contour measurements differ from radiographic ones. That distinction returns in the section on how PosturaScreen estimates pelvic tilt from photos.
How common it is
A casual look around any gym, office, or family gathering reveals an obvious truth: pelvic tilt sits on a spectrum, and the exact neutral pelvis is statistically rare. A review in the International Journal of Sports Physical Therapy examined clinical measures of pelvic tilt and reported wide variation across healthy adult populations, with most people falling somewhere on a small bias toward anterior or posterior tilt rather than landing on a textbook-neutral position.
That observation matters for how to read a photograph. Seeing a few degrees of backward pelvic rotation in a side photo does not, on its own, mean anything is wrong. This is a relatively common finding and is often asymptomatic, but it should be interpreted together with the full clinical picture. A person with a visible PPT signal and no pain, no movement limitations, and no functional concerns is statistically closer to the norm than to an outlier.
Where PPT becomes more meaningful is when the visual signal is strong (a clearly flattened lower back, with the hips visibly tucked under the body on a side photo) AND it co-occurs with persistent low-back pain, stiffness, or movement restrictions. In those situations the photo serves as one data point in a broader conversation — never the diagnosis itself.
Several factors are commonly associated with PPT in observational studies: prolonged slumped sitting, habitual posterior tucking of the pelvis, and certain patterns of muscle length around the hip. Whether any of these cause PPT in any given person is a research question that goes beyond a postural photograph. For most practical purposes, the right mindset is: common postural pattern, sometimes worth a closer clinical look, often worth nothing more than noticing.
What PPT looks like in 2D photos
The most reliable place to spot posterior pelvic tilt is a side-view photograph taken at roughly hip height, with the whole body in frame and a clean background behind the subject. From that angle, four visual signs tend to appear together when PPT is present.
The first is a flattened curve in the lower back. In a neutral side view, the lower spine shows a gentle inward curve — the natural lumbar lordosis. With PPT, that curve becomes noticeably shallower, sometimes described colloquially as a “flat back” or “ironed-out” lower spine. The small hollow above the buttocks looks reduced or nearly absent when the subject stands still.
The second sign is the waistline angle. If the subject is wearing pants or shorts with a defined waistband, that band tilts upward and forward at the front in someone with PPT, rather than running horizontal to the floor. Looking at a side photo, the front of the belt or waistband sits higher than the back — the mirror image of what anterior tilt produces. The angle is subtle but consistent.
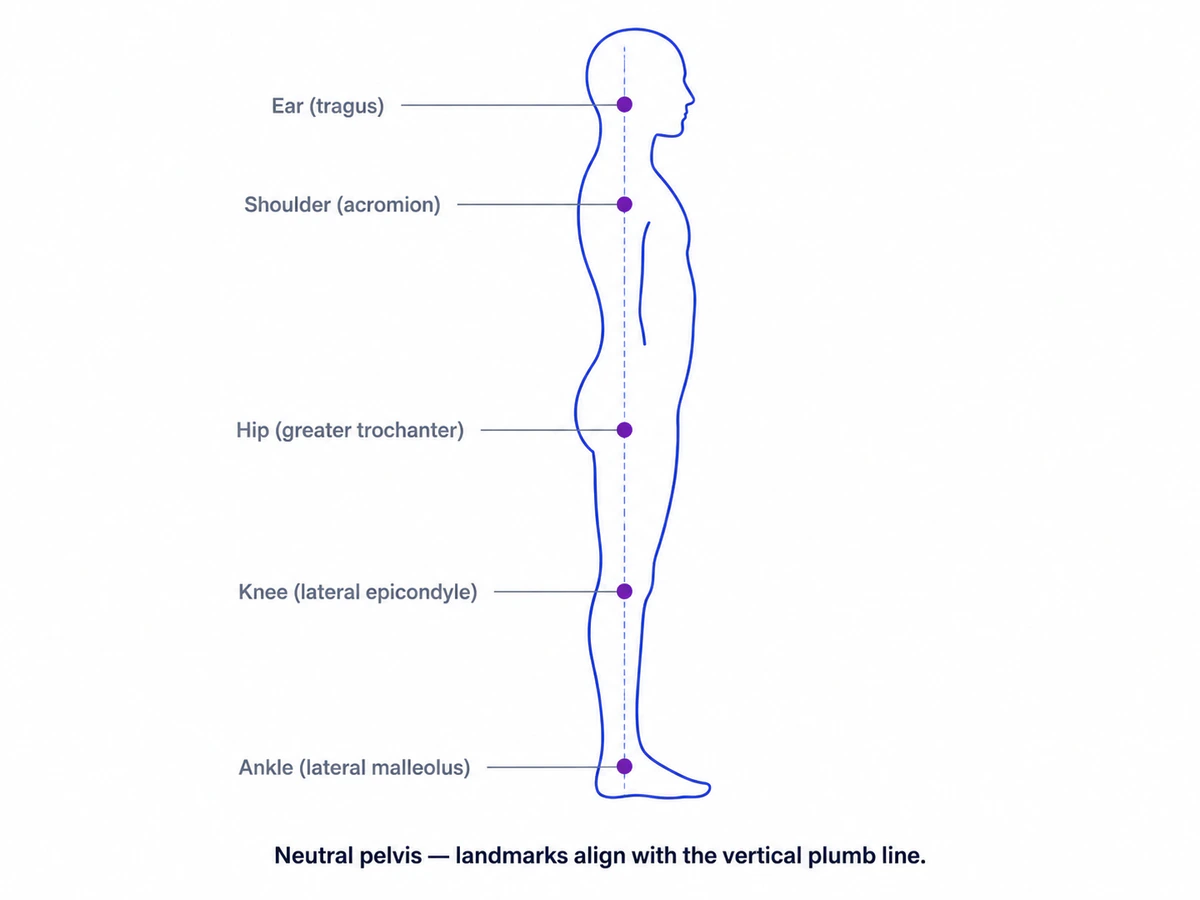
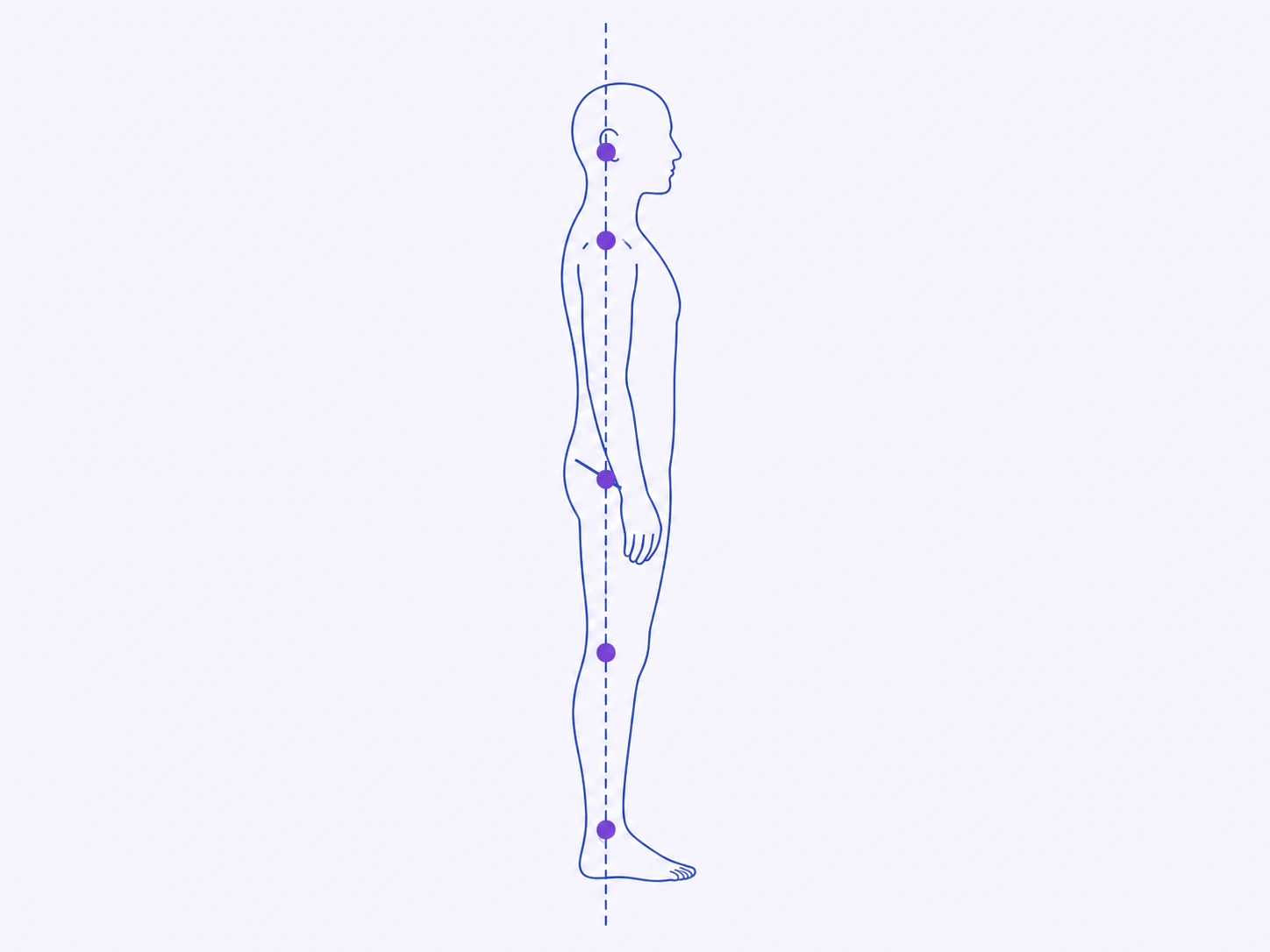
The third sign is hip position relative to the shoulder line. In a neutral standing posture, a plumb line dropped from the ear should pass close to the shoulder, the hip joint, the knee, and the ankle. With PPT, the hips tuck under and sit beneath or slightly behind that plumb line, while the upper body may drift into a gentle slump above them. The result is a side view where the pelvis appears tucked under the torso rather than leading it.
The fourth sign is a flattened, tucked-in appearance of the buttocks. When the pelvis rotates backward, the buttocks rotate downward and under, so they project less behind the body. For lean people this often looks like a “tucked” or flattened seat. For larger people, the same rotation makes the buttocks sit lower and tighter against the back of the legs rather than projecting backward.
Several common photo conditions distort or hide these signs. A camera held above hip height makes the pelvis look more tucked than it is; a camera below hip height can hide the flattening. Loose drape-style clothing hides the waistline angle entirely. Photos taken from a slight three-quarter angle rather than a true side view make the comparison to a plumb line unreliable. The next section on capture protocol covers how to avoid these errors.
It is worth emphasizing what these visual signs are not. They are not a measurement of any underlying skeletal angle the way a radiograph would measure it. They are surface-contour patterns that suggest the underlying pelvic rotation. Clothing, body composition, breathing phase, and the moment when the photo is captured all influence what shows up. The visual signal is genuinely useful, especially for trending over time in the same person under the same conditions — but it is a screening signal, not a diagnostic measurement.
Across the four visual signs, the flattened lower-back curve is the most reliable single indicator on a clean side photo. The other three reinforce the picture. When all four appear together, the PPT pattern is unambiguous. When only one or two appear, the case is weaker and other interpretations are possible.
PPT vs APT — at a glance
Posterior pelvic tilt is one end of a small spectrum. The other end is anterior pelvic tilt (APT), where the pelvis rotates forward, the lower back arches, and the buttocks stick out. A neutral pelvis sits in between, with a normal but not exaggerated lower-back curve.
Most people in everyday photographs do not show a pure example of any one pattern. A small bias toward PPT or toward APT is the norm. Pure PPT or pure APT — extreme rotation in either direction — is uncommon in healthy adults outside of athletic, occupational, or post-injury contexts. The summary below (adapted from Ivy Rehab’s clinical breakdown) is meant for orientation: actual photos rarely fit any single column perfectly, and small mixes are common.
| Posterior pelvic tilt Tipped back | Neutral Aligned | Anterior pelvic tilt Tipped forward | |
|---|---|---|---|
| Lower-back arch | Flat | Normal curve | Pronounced |
| Hip position (side view) | Tucked under shoulders | Aligned with shoulders | Forward of shoulders |
| Buttocks appearance | Tucked under | Normal | Sticks out |
| Lumbar curve | Hypolordosis or flat | Neutral lordosis | Hyperlordosis |
The takeaway: knowing where someone sits on this spectrum is more useful than placing them in a category. A person whose photo signals “slightly posterior” is not in the same situation as someone whose photo signals “strongly posterior with pain and stiffness.” For the opposite pattern and how it appears in photos, see the companion guide on anterior pelvic tilt.
How to take a side photo to see your own pelvic tilt
A photograph that reliably reveals pelvic tilt follows a short capture protocol. Most distortion comes from the camera, not from the body — small changes in camera height, angle, or distance can make the same person look more or less tilted than they actually are.
The protocol is straightforward:
- Background. Stand against a plain wall or a flat surface free of clutter. Avoid backgrounds with horizontal lines that compete visually with the waistline.
- Body position. Stand sideways to the camera, weight evenly distributed on both feet, arms relaxed at the sides. Avoid pressing the arms against the hips or putting hands in pockets. Look straight ahead, not down or up.
- Camera position. The camera should sit at approximately hip height, not above or below. A tripod or a stack of books works. A phone propped against something stable is fine.
- Camera distance. Two to three meters away. Closer than that introduces lens distortion that exaggerates whichever body part is closest to the camera.
- Framing. The whole body should be in the frame, with the hip approximately in the vertical center of the photo. Heads cut off, feet cut off, or hips off-center will make later comparisons unreliable.
- Camera level. Use a phone’s built-in level indicator or a level app. A tilted camera makes every angle in the photo unreliable.
- Clothing. Close-fitting, athletic, or undergarments work best. Loose drape clothing hides the waistline angle and the lower-back curve. The goal is to see body contours, not fabric drape.
- Pose. Stand naturally. “Performing good posture” defeats the point of the photograph. Stand the way you stand when you are not thinking about it.
Two side photos — one of each side — give a more complete picture than a single side. Some people have a small asymmetry that shows up on one side but not the other. Taking both sides also helps catch capture errors: a single mis-leveled photo will look very different from the matching side taken correctly.
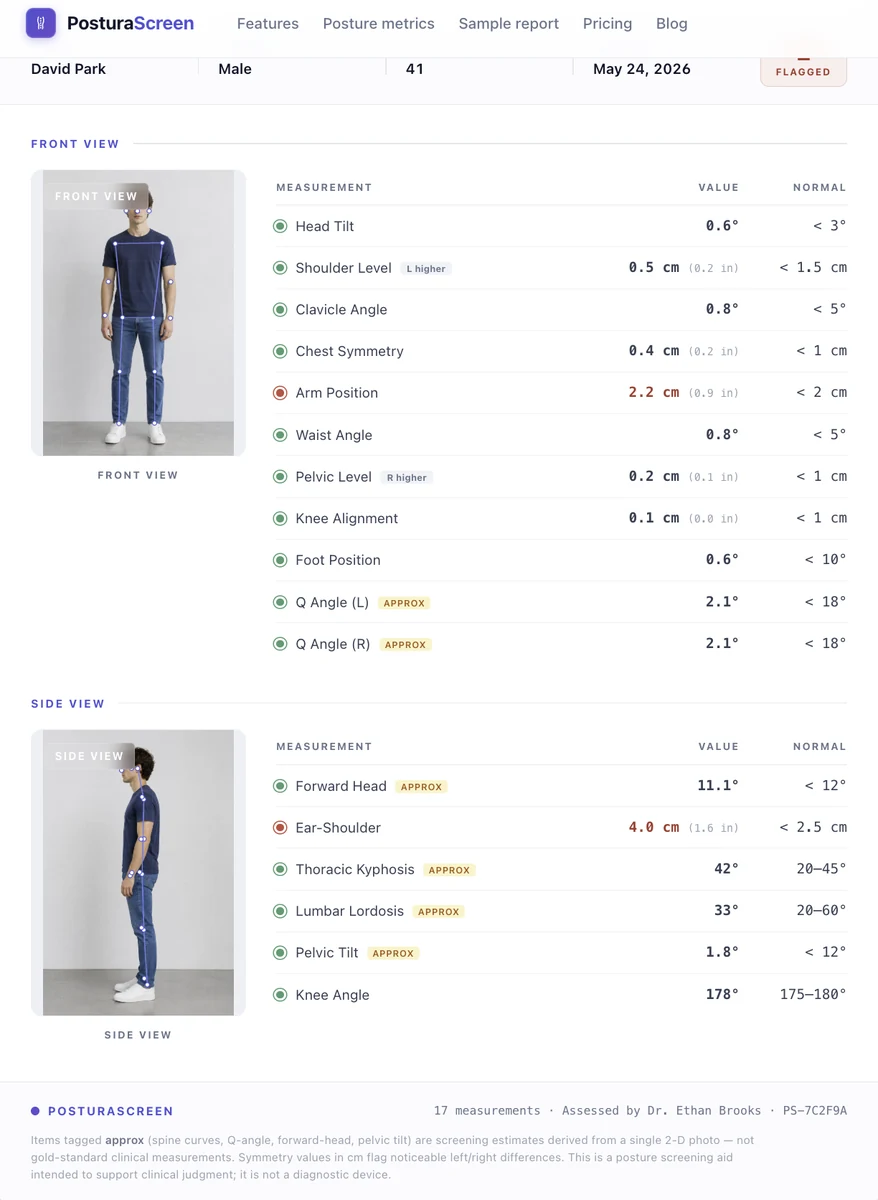
For self-screening, taking the same set of photos every few weeks under the same conditions is more informative than a single grade. The PosturaScreen sample report shows what a clinical report based on this kind of capture looks like, and the methodology page documents how each metric is computed from the keypoints in the photo.
Three common mistakes account for most “my photo looks weird” results: (1) the camera was held by another person at chest height instead of being mounted at hip height; (2) the subject was wearing baggy or wrinkled clothing; (3) the subject “fixed” their posture before the photo was taken. Re-shooting under controlled conditions usually resolves these.
How PosturaScreen estimates pelvic tilt from photos
PosturaScreen, the product behind this article, estimates a sagittal pelvic tilt signal from a single side-view photo. The calculation is deterministic and geometric: a vector is drawn from the hip keypoint to the knee keypoint, and the angle between that vector and a vertical reference line is reported as an approximate pelvic tilt angle, in degrees. Posterior and anterior tilt appear as opposite directions of the same signal. The system does not measure the true pelvic bone angle; it estimates a 2D posture signal from visible surface landmarks.
approx because 2D photo measurements differ from radiographic ones. Posterior tilt registers as the opposite direction of anterior tilt on the same scale.In every report, this metric carries an approx tag. The tag is honest about what the number represents. The geometric calculation reliably captures the surface relationship between the hip and the leg in the photo. It does not capture the underlying skeletal pelvic tilt the way a radiograph would, because surface contour is influenced by clothing, body composition, breathing phase, and small variations in how the subject was standing at the moment of capture. The reading is best used to compare the same person over time under similar photo conditions, not to grade absolute clinical severity between individuals.
The practical value of this number is not absolute clinical grading. The practical value is trending in the same person under consistent capture conditions. A pelvic tilt reading today is not directly comparable to someone else’s reading taken under different conditions, but it is comparable to that same person’s reading six weeks later, if both photos were taken with the same setup.
That is how PosturaScreen tends to be used in practice: as a screening signal that initiates a conversation, and as a tracking signal that flags change over time. The full mathematical definition of every metric, including pelvic tilt, lives on the PosturaScreen methodology page. The 17 posture metrics that go into a standard report, including pelvic tilt, are documented there as well.
When to talk to a clinician about posterior pelvic tilt
A side photo with a visible PPT signal does not require a clinical visit on its own. As noted earlier, some degree of pelvic tilt is the norm. A visible PPT pattern in a photo can appear in people with or without symptoms; by itself, the photo finding does not prove the posture is painful, harmful, or clinically significant.
The signal becomes worth a clinician’s attention when it co-occurs with one or more of the following:
- Persistent low-back, hip, or knee pain that does not resolve with simple rest or that recurs with activity.
- Movement limitations — difficulty walking comfortably, running without discomfort, squatting through a full range of motion, or sitting for normal periods.
- Recent change — a visible PPT signal that was not previously present, especially after an injury or a significant change in activity level.
- Postural concerns paired with neurological symptoms — any numbness, weakness, or radiating pain. These warrant clinical evaluation independent of the PPT signal.
Several professional groups are positioned to integrate a photo signal with the rest of someone’s clinical picture: licensed physiotherapists, chiropractors, sports-medicine physicians, and orthopedic specialists. They can perform a physical examination, take a history, and decide whether the postural pattern observed in a photograph is worth further investigation, treatment, or simply monitoring over time. OrthoInfo from the American Academy of Orthopaedic Surgeons is a reasonable starting point for understanding when persistent musculoskeletal concerns warrant clinical evaluation.
What a photograph cannot do is replace any of that. A photograph is a snapshot of surface contour at a moment in time. It does not measure pain. It does not measure strength. It does not measure tissue health. It does not capture the dozens of other things a clinician integrates into an assessment.
PosturaScreen is built as a screening and tracking tool. It is not a diagnostic device, and it does not provide medical advice. The information in this article is educational. For specific concerns about posture or musculoskeletal health, the right next step is a conversation with a qualified healthcare professional.
Frequently asked questions
What does posterior pelvic tilt look like?
From the side, posterior pelvic tilt produces a flattened lower back that loses its natural inward curve, a waistline that tilts upward at the front, hips that tuck under the body, and buttocks that appear flat or tucked in rather than projecting. The most reliable visual sign is the flattened lower-back curve — noticeably less arch than a neutral standing posture.
How can someone tell if they have posterior pelvic tilt?
Stand side-on against a clean wall and take a full-body photo. Look for the four signs above — flattened lower-back curve, an upward-tilting waistline, hips tucked under, and flat-looking buttocks. A quick low-tech check: stand against a wall with heels and shoulders touching; with posterior tilt, the lower back presses flat against the wall with almost no gap behind it.
Is posterior pelvic tilt bad?
Posterior pelvic tilt is a postural pattern, not a diagnosis. This is a relatively common finding and is often asymptomatic, but it should be interpreted together with the full clinical picture. PPT becomes worth clinical attention when it occurs alongside pain, stiffness, or movement restrictions. A photograph alone cannot determine whether anyone’s PPT is medically significant — that judgment belongs to a clinician.
What’s the difference between posterior and anterior pelvic tilt?
Posterior pelvic tilt: pelvis tips backward, the lower back flattens, hips tuck under, buttocks appear tucked in. Anterior pelvic tilt: pelvis tips forward, the lower-back curve is pronounced, hips appear ahead of the shoulders, buttocks tend to stick out. Pure PPT or pure APT is rare; most people have a small bias one direction or the other.
Can a 2D photo really measure pelvic tilt?
A 2D side photo reliably shows the appearance of pelvic tilt. It does not measure the underlying skeletal pelvic tilt the way a radiograph does, because surface contour is influenced by clothing, body composition, and breathing phase. Photo-based pelvic tilt readings are best used for tracking change in the same person over time, not for comparing absolute numbers between people. That is why PosturaScreen tags this metric approx in every report.
When should someone see a clinician about posterior pelvic tilt?
When a visible PPT signal in side photos occurs alongside ongoing pain, stiffness, or movement limitations in the lower back, hips, or knees, it is worth consulting a licensed physiotherapist, physician, or chiropractor. They can integrate the photo signal with a physical examination and history to decide if anything needs intervention. PosturaScreen is a screening and tracking tool, not a diagnostic device.
This article was prepared by the PosturaScreen editorial team for posture education. It is not medical advice and is not a substitute for a clinical evaluation. PosturaScreen is a screening and tracking tool, not a diagnostic device. If you have concerns about your posture or musculoskeletal health, consult a licensed healthcare professional. See our editorial standards for how this article was written and reviewed.