Uneven Shoulders & Hips: What Asymmetry Looks Like in Photos
Posture asymmetry refers to visible left-right differences in how the body sits — uneven shoulders with one higher than the other, a hip that rides up on one side, a head that tilts slightly, or knees that track differently. In a front-view photo, these show up as height and angle differences between the left and right sides. Small left-right differences are extremely common and are usually asymptomatic; near-perfect symmetry is the exception, not the rule. A photo finding alone does not establish whether any asymmetry is meaningful. This guide explains what posture asymmetry looks like in a front photo, why some asymmetry is normal, how it differs from muscle imbalance and scoliosis, and when the photo signs are worth discussing with a clinician.
- Posture asymmetry means visible left-right differences: uneven shoulders, uneven hips, head tilt, and differences in knee tracking (Q-angle).
- The best way to see it is a front-view full-body photo with the camera at hip height, level, and centered — not angled up or down.
- Small asymmetries are the norm, not a problem. Handedness, which arm carries the bag, and which leg you stand on all create everyday left-right differences.
- ”Posture asymmetry” is what a photo can show. It is not the same as muscle imbalance (a strength difference, not visible in a photo) or scoliosis (a clinical spinal diagnosis).
- A notable or progressing asymmetry — especially a new one, or one in a child or adolescent — is worth discussing with a licensed physiotherapist, physician, or chiropractor.
What posture asymmetry is (and what it is not)
Posture asymmetry describes a visible difference between the left and right sides of the body when viewed from the front. The most common signs are a shoulder that sits higher on one side, a hip that rides up, a head that tilts slightly, and knees that angle differently. These are differences in the frontal plane — the side-to-side dimension you see when someone faces you directly — as opposed to the front-to-back patterns seen from the side, such as anterior pelvic tilt or tech neck.
It helps to separate three terms that often get blurred together, because they mean genuinely different things.
Posture asymmetry is a visible, geometric left-right difference that a photograph can show. It is an observation, not a diagnosis.
Muscle imbalance is a difference in strength or activation between muscles on the two sides, or between opposing muscle groups. A photograph cannot measure strength, so it cannot measure muscle imbalance. Assessing that requires functional testing or a clinical examination. The two can be related — but a visible asymmetry does not prove a strength difference, and a strength difference does not always produce a visible asymmetry.
Scoliosis is a clinical diagnosis: a sideways curvature of the spine confirmed by a healthcare professional through physical examination and imaging. A front photo cannot diagnose scoliosis. A visible asymmetry can be one screening sign among several, but the diagnosis belongs to a clinician.
Throughout this article, the focus stays on the first of these — what a front-view photo can actually show. PosturaScreen, the product behind this blog, reports the visible left-right differences from photo landmarks and does not claim to assess muscle strength or to diagnose any spinal condition.
Uneven shoulders — what it looks like from the front
A shoulder-height difference is the most recognizable sign of posture asymmetry, and the one people most often notice in their own photos. In a front-view image, it shows up as a tilt in the line connecting the two shoulder points: one shoulder sits higher, the other lower.
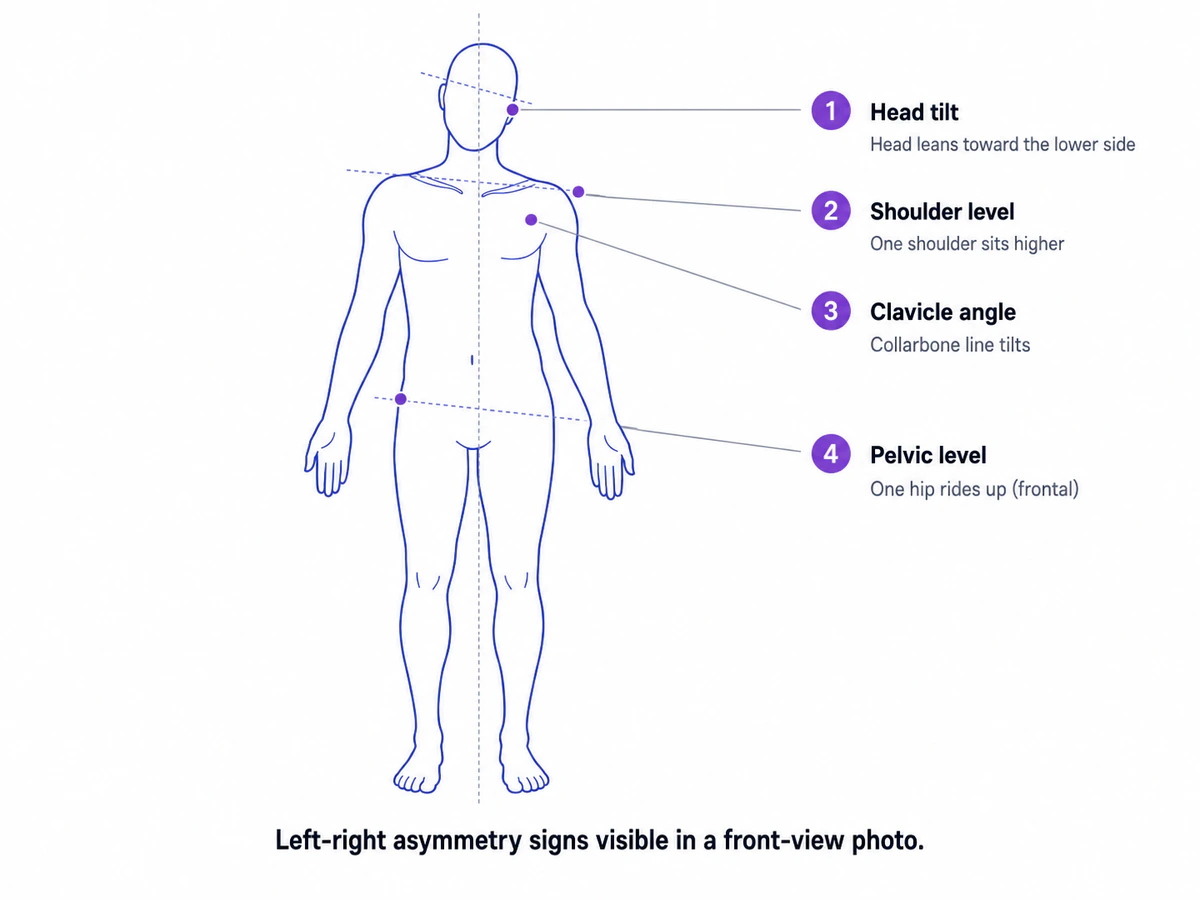
Three signs commonly travel together in the upper body. Shoulder level is the vertical difference in height between the two shoulders. Clavicle angle is the tilt of the collarbone line, which usually shifts in the same direction as the shoulder difference. Head tilt is a slight lean of the head toward the lower shoulder, a natural way the body keeps the eyes level when the shoulders are uneven.
Most everyday shoulder asymmetry comes from ordinary causes rather than anything concerning: handedness, consistently carrying a bag on one shoulder, the way a person sits at a desk, or which leg they habitually stand on. None of these are diagnoses, and a photo cannot establish which cause applies — it can only show the difference.
One technical point worth understanding: among the front-view metrics, the left-right symmetry measures — shoulder level, clavicle angle, head tilt, and pelvic level — are not tagged approx in a PosturaScreen report. Comparing two landmarks at the same depth (the left shoulder against the right shoulder) is more directly measurable from a 2D photo than estimating a spine curve, which has to infer depth. These front-view symmetry metrics are among the more reliable numbers in a photo-based screen.
Uneven hips and lateral pelvic tilt
The same left-right logic applies to the pelvis. When one hip rides higher than the other in a front-view photo, the line connecting the two hip points tilts — a pattern clinicians call lateral pelvic tilt, and that many people describe informally as a “hip hike.” PosturaScreen reports this as Pelvic Level, the vertical difference between the left and right hip landmarks, with a normal range under one centimeter.
It is worth being precise here, because the pelvis can be described in two completely different ways depending on the viewing plane. Lateral pelvic tilt is the frontal (side-to-side) difference seen from the front. That is different from anterior pelvic tilt — the front-to-back rotation seen from the side, covered in the anterior pelvic tilt guide. A person can have one, both, or neither. The two are measured from different photos and describe different things.
Common everyday contributors to a visible hip-height difference include standing with weight on one leg, habitual carrying patterns, and small natural differences in leg length. Leg-length differences in particular are worth flagging to a clinician if they appear significant, because the assessment and interpretation of limb-length differences is a clinical matter rather than something a photo can settle.
Knee tracking differences (Q-angle, left vs right)
Asymmetry is not limited to shoulders and hips. The knees can track differently on the two sides, and a front-view photo can show this through the Q-angle — the angle formed by the line from the hip to the center of the knee, and from the knee to the ankle. PosturaScreen reports a Q-angle for each leg, with a typical screening range under roughly 18° for men and 22° for women.
Unlike the shoulder and hip level measurements, the Q-angle carries an approx tag. The reason is depth: estimating the hip-knee-ankle angle from a flat photo involves inferring positions that are not all at the same distance from the camera, so it is a screening estimate rather than a direct comparison of two same-depth landmarks. A difference between the left and right Q-angle is one more asymmetry signal, useful for screening and for tracking change over time rather than for clinical grading.
When knee tracking looks notably different between the two sides, or when it occurs alongside knee pain, the right step is a clinical assessment. OrthoInfo from the American Academy of Orthopaedic Surgeons is a reasonable starting point for understanding when knee-alignment concerns warrant evaluation.
Symmetry is a spectrum — and how to take a usable front photo
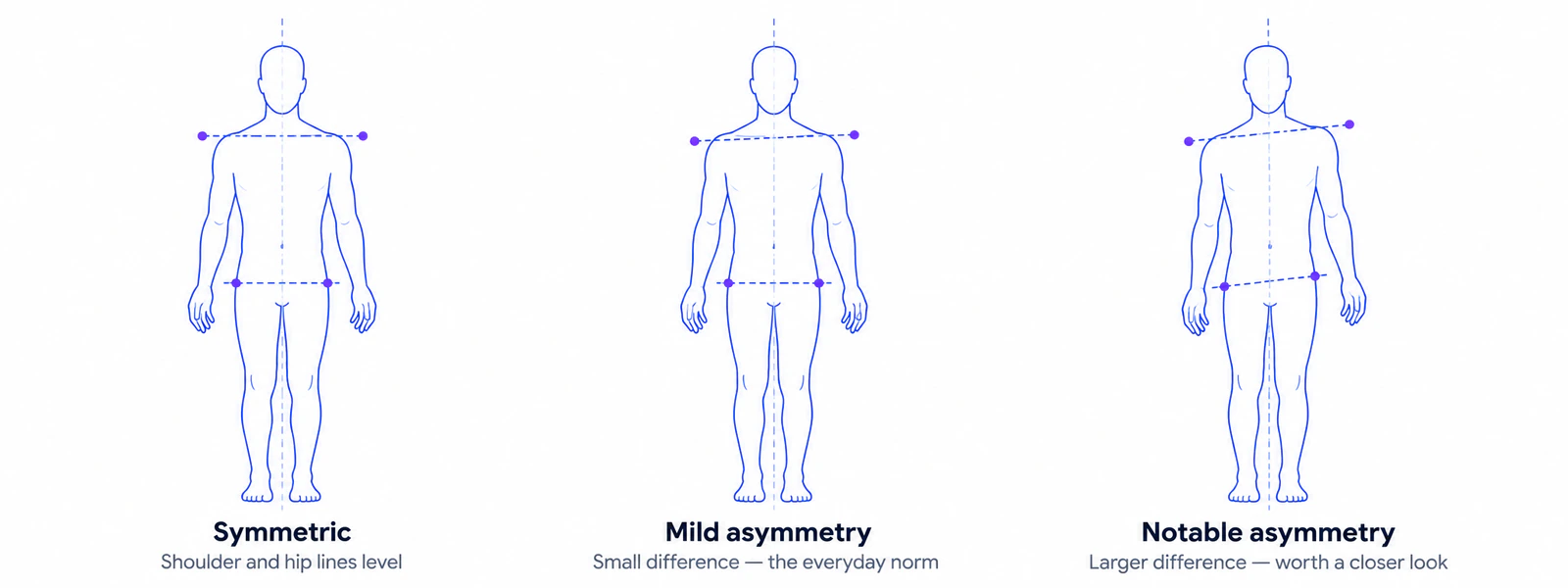
Before reading any front-view photo, it helps to set expectations: perfect symmetry is rare. Posture asymmetry sits on a spectrum, with most people showing a small left-right difference that is entirely normal.
The setup matters more than the equipment. Stand facing the camera head-on, with the camera mounted at hip height and perfectly level — not angled up or down. A camera that tilts even slightly will exaggerate or invent an asymmetry that is not really there, which is the single most common source of misleading front-view photos. Use a plain wall, wear fitted clothing so the shoulder and hip contours are visible, stand with feet about shoulder-width apart and weight even on both legs, and let the arms hang naturally. Do not consciously “straighten up” before the shutter clicks; the goal is to record the default standing posture, not a corrected one.
A notable asymmetry deserves a closer look — and in some situations, a clinician’s assessment. It is worth consulting a licensed physiotherapist, physician, or chiropractor when an asymmetry is notable, new, or progressing; when it occurs alongside pain, stiffness, or restricted movement; or when there is any numbness, tingling, or weakness, which are neurological signals that warrant prompt evaluation regardless of posture. One situation deserves particular attention: a new or progressing asymmetry in a child or adolescent. Scoliosis screening in young people is a routine clinical matter, and a visible asymmetry in that age group is best evaluated by a healthcare professional rather than interpreted from a photo. The Cleveland Clinic provides accessible background on when uneven shoulders warrant medical attention.
How PosturaScreen measures left-right asymmetry from photos
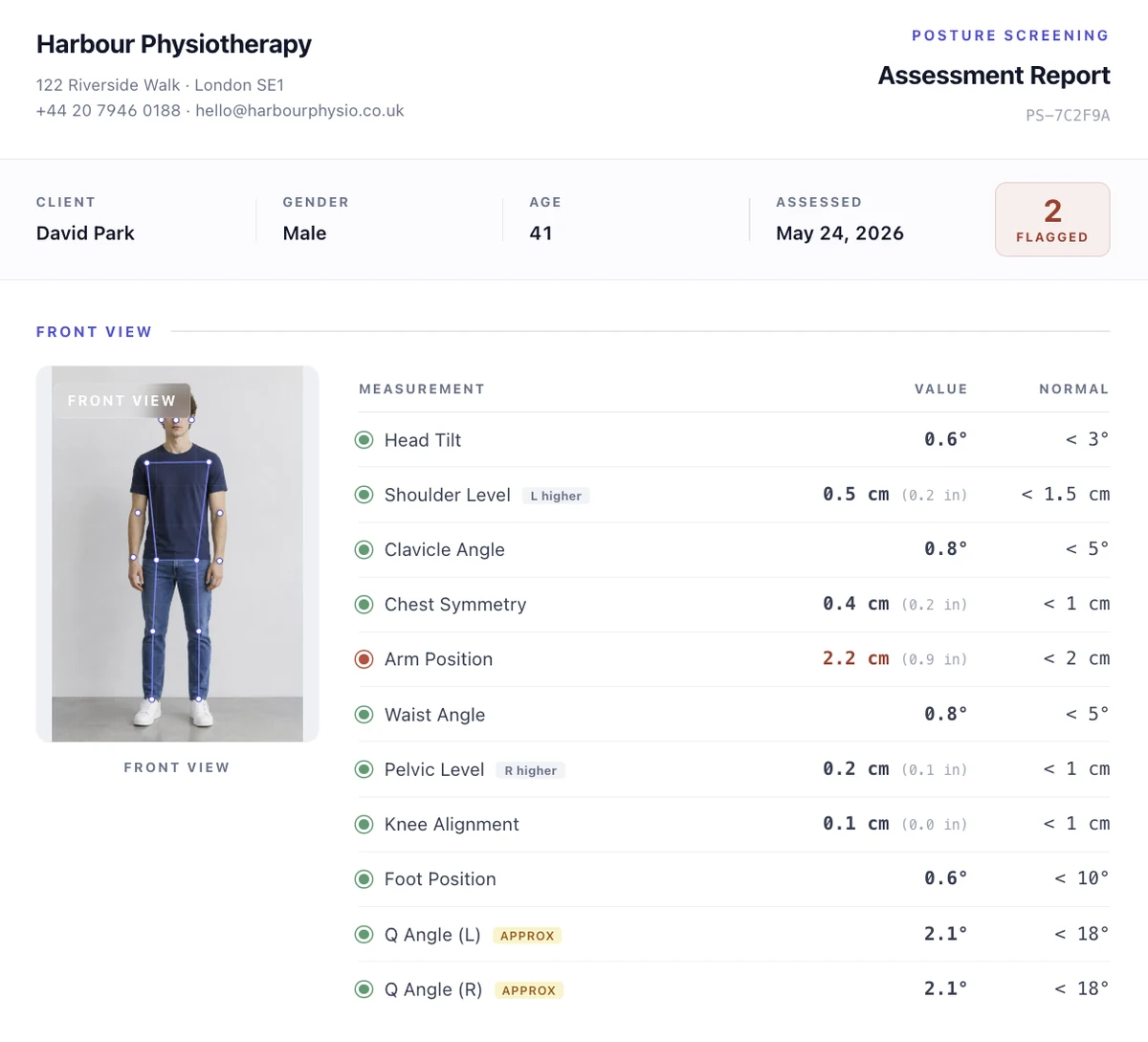
PosturaScreen, the product behind this article, computes a set of front-view symmetry metrics directly from a single front-facing photo: Head Tilt (normal under 3°), Shoulder Level (the vertical difference between the shoulders, normal under 1.5 cm), Clavicle Angle (normal under 5°), Pelvic Level (the frontal hip-height difference, normal under 1 cm), and Q Angle for each leg (a screening range under roughly 18° for men and 22° for women).
approx tag.There is an important distinction in how confident these numbers are. Unlike the sagittal spine curves measured from a side photo, most front-view symmetry metrics are not tagged approx: comparing two landmarks at the same depth — the left shoulder height against the right — is more directly measurable from a 2D photo than estimating a spine curve, which has to infer depth. The Q-angle remains approx because it involves that depth inference. This is why the same report can show a directly-measured Shoulder Level alongside an estimated Q-angle.
The practical value of these numbers is tracking. A shoulder-level difference of 1.8 cm today is most useful when compared to that same person’s measurement six weeks later, taken with the same camera setup, after a change in habits like switching the bag-carrying side or adjusting a workstation. That is how PosturaScreen tends to be used in practice: as a screening signal that initiates a conversation, and as a tracking signal that flags change over time. The full mathematical definition of each metric lives on the methodology page, and the sample report shows what a complete front-view readout looks like.
To be clear about the boundary: PosturaScreen reports the visible left-right differences in a photo. It does not assess muscle strength or activation, and it does not diagnose scoliosis or any spinal condition. It is a screening and tracking tool, not a diagnostic device. For specific concerns about posture or musculoskeletal health, the right next step is a conversation with a qualified healthcare professional.
Frequently asked questions
Why is one shoulder higher than the other?
A shoulder-height difference in a front-view photo usually reflects everyday factors: handedness, the side you carry a bag on, how you sit, or which leg you tend to stand on. Small differences are extremely common and typically asymptomatic. A photo can show the difference but cannot explain the cause on its own. If it is notable, new, or accompanied by pain or stiffness, a licensed physiotherapist, physician, or chiropractor can assess it properly.
Are uneven shoulders or hips normal?
Small left-right asymmetries are the norm, not the exception. Near-perfect symmetry is rare, and most people show a slight difference in shoulder height, hip height, or head position. By itself, a visible asymmetry in a photo does not prove anything is wrong. It becomes worth a clinician’s attention when it is notable, when it is new or progressing, when it occurs alongside pain, or when it appears in a child or adolescent.
Is posture asymmetry the same as scoliosis?
No. Posture asymmetry is a visible left-right difference that a photo can show. Scoliosis is a clinical diagnosis of a sideways curvature of the spine, confirmed through physical examination and imaging by a healthcare professional. A front photo cannot diagnose scoliosis. A visible asymmetry can be one of several screening signs, but the diagnosis itself belongs to a clinician — especially for children and adolescents, where scoliosis screening is a routine clinical matter.
Is posture asymmetry the same as muscle imbalance?
No. Posture asymmetry is a geometric, visible difference between the left and right sides that shows up in a photo. Muscle imbalance refers to a difference in strength or activation between muscles — something a photo cannot measure, and which requires functional testing or clinical assessment. The two can be related, but they are not the same thing. PosturaScreen reports the visible asymmetry; it does not assess muscle strength or activation.
Can a 2D photo track posture asymmetry over time?
Yes — that is the strongest use case. A front-view photo taken under consistent conditions (camera level, same height, same distance, same stance) lets a person see whether a shoulder-height or hip-height difference is increasing, stable, or decreasing over weeks. PosturaScreen reports Shoulder Level, Pelvic Level, Head Tilt, and Clavicle Angle directly from the photo; most of these are not tagged approx because comparing two landmarks at the same depth is more directly measurable than estimating a spine curve.
When should someone see a clinician about posture asymmetry?
When an asymmetry is notable, new, or progressing; when it occurs alongside pain, stiffness, or restricted movement; when it appears in a child or adolescent; or when there is any numbness, tingling, or weakness, it is worth consulting a licensed physiotherapist, physician, or chiropractor. They can integrate the photo signal with a physical examination and history. PosturaScreen is a screening and tracking tool, not a diagnostic device.
This article was prepared by the PosturaScreen editorial team for posture education. It is not medical advice and is not a substitute for a clinical evaluation. PosturaScreen is a screening and tracking tool, not a diagnostic device. If you have concerns about your posture or musculoskeletal health, consult a licensed healthcare professional. See our editorial standards for how this article was written and reviewed.